It’s been just over 2 years since we published our first COBRA-OS® study, “Size Matters; first-in-human study of a novel 4 French REBOA device.” Since that study, I have personally been using the device clinically and have been hearing stories about the COBRA-OS® from customers all over North America and beyond.
I have been overwhelmed by the usefulness of this tool and specifically how much it has anecdotally improved access site complications. I remember using previous larger profile devices and was always concerned with thrombotic complications but now, it barely enters my mind. As a vascular surgeon, I know that the endovascular device profile is vitally important and is directly linked to arterial access complications. As co-founder of Front Line Medical Technologies, it was the driving force behind developing a much lower profile REBOA device in order to minimize these complications.
Recently, there was an excellent systematic review and meta-analysis of lower extremity vascular complications after arterial access for Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) by Power Foley and colleagues1. They raised the important question of whether having access site complications was “an inevitable concern?” in the goal of preserving life over a limb with REBOA. The authors focused on the data derived from the 7 French or larger devices that have been used in the past. However, the authors did not recognize in their discussion that arterial access complications might further be reduced if even lower profile REBOA devices than 7 French are used.
Borrowing from the vascular surgery literature, the largest review of femoral access site complications in peripheral vascular interventions was published in 2014 using data from the multicenter Vascular Quality Initiative in over 27,000 femoral access procedures2. This study clearly showed that there was an increase in complications using sheaths larger than 6 French. In practice, this is why most vascular surgeons will use a vascular closure device to help prevent complications (instead of simply using manual compression) when using a 7 French sheath but often do not when using a 6 French sheath. There is a “chasm” between 6 and 7 French systems in vascular surgeons’ brains. I am therefore not overly surprised that Power Foley did not find any difference between the 7 French and >10 French groups in terms of complications, which occur almost once in every 10 patients (8.6%).
Note: A vascular closure device is usually a piece of collagen, clip, or suture meant to provide immediate sealing of the arterial puncture after an access procedure that removes the need for manual compression, which can take up to 30 minutes depending on the size of the sheath. There are about 15 devices on the market. Guess how many are designed to close 7 French sheaths? All of them. Guess how many are meant to close 4 French sheaths? None of them. 4 French is literally too small to even need a closure device!
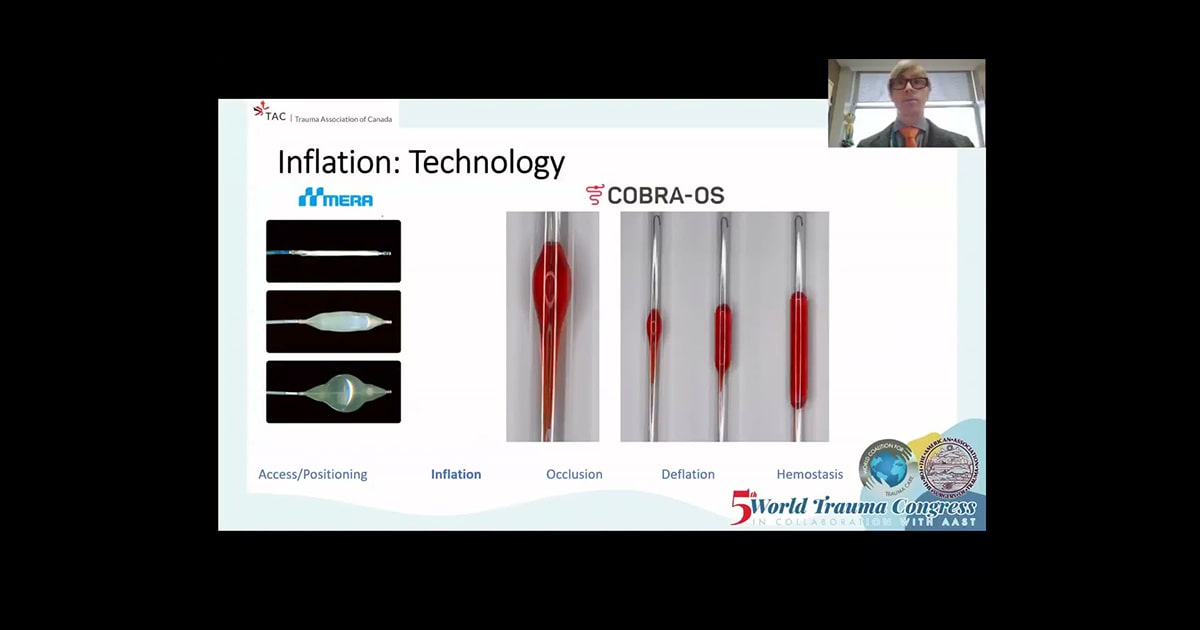
I agree with the authors that there are likely two levels of occlusion that are contributing to these complications, firstly the intended aortic occlusion and secondly the outflow obstruction caused by the access sheath. However, it is important to realize that when patients have access site complications, the vast majority occur in the ipsilateral access site limb and not bilaterally. Therefore, access sheath obstruction is the most important factor. With a normal common femoral artery being around 6 mm in diameter and even smaller in hypotensive trauma patients whose blood vessels are vasospastic, every sheath mm reduction matters (4 French 1.5 mm; 7 French 2.5 mm) when considering collateral flow and reducing thrombotic complications.
If REBOA was easy and free of complications, there would be less controversy about its value in non-compressible torso trauma. Since REBOA is not free and can lead to serious sequelae, it is important to reduce the risks as much as possible to maximize the potential benefits. Whether working in the medical device industry or on the clinical front lines treating patients, we should never accept complications as “inevitable” while we are investigating and implementing new treatments for our patients.
1. Power A, Parekh A, Scallan O, et al. Size matters: first-in-human study of a novel 4 French REBOA device. Trauma Surgery & Acute Care Open 2021;6:e000617. doi: 10.1136/tsaco-2020-000617
1. Foley MP, Walsh SR, Doolan N, Vulliamy P, McMonagle M, Aylwin C. Systematic Review and Meta-Analysis of Lower Extremity Vascular Complications after Arterial Access for Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA): An Inevitable Concern? Eur J Vasc Endovasc Surg. 2023 Feb 14:S1078-5884(23)00130-2. doi: 10.1016/j.ejvs.2023.02.007. Epub ahead of print. PMID: 36796674.
2. Ortiz D, Jahangir A, Singh M, Allaqaband S, Bajwa TK, Mewissen MW. Access site complications after peripheral vascular interventions: incidence, predictors, and outcomes. Circ Cardiovasc Interv. 2014 Dec;7(6):821-8. doi: 10.1161/CIRCINTERVENTIONS.114.001306. Epub 2014 Nov 11. PMID: 25389345; PMCID: PMC4529288.