Disclaimer: As an academic vascular surgeon having run and participated in multiple randomized controlled trials in the past, this commentary is not meant to devalue the hard work and good intentions of the UK-REBOA Trial investigators. It is primarily meant for those who are already negatively biased toward REBOA (most of whom have never performed REBOA) and are using the UK-REBOA trial as confirmation of their preconceived notions. This commentary is also based solely on the slides presented at the recent Critical Care Reviews (CCR) 2023 Conference and shared on Twitter. I anxiously await the full published results.
Questions that I had after seeing the grainy Twitter slides from #CCR2023:
- Why is it taking so long for them to get the patient to a definitive hemorrhage control procedure?
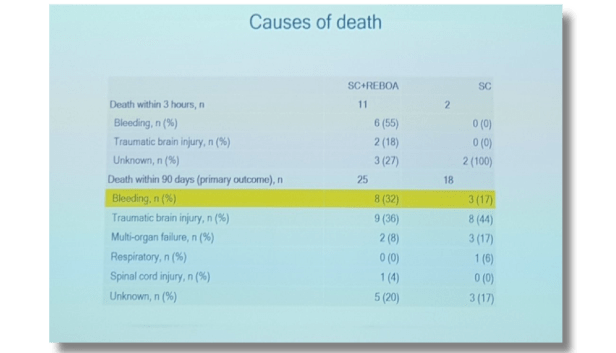
- Why are almost half of the patients in this trial dying from hemorrhage but most not even going to the OR to attempt definitive hemorrhage control?
- Wait a second… 16 Trial sites and only 19 balloon inflations? Did any single surgeon even perform REBOA more than once in this trial?
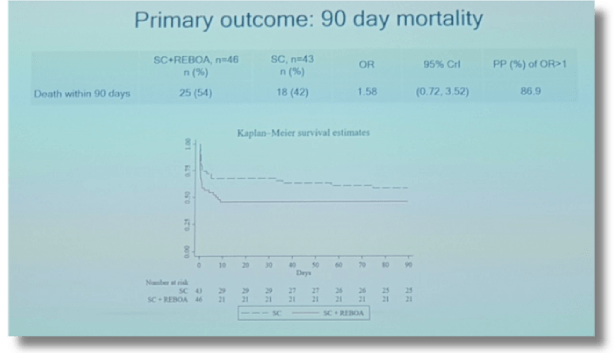
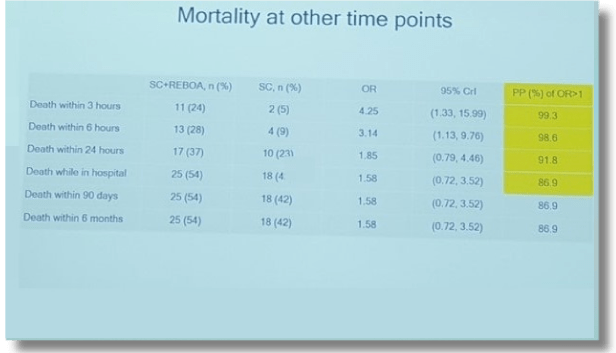
According to these now infamous Twitter slides, 54% of REBOA patients and 42% of standard care patients died without leaving the hospital and most patients in both groups died of hemorrhage. Thus, almost 1 in 2 patients bled to death in this study regardless of whether REBOA was used or not.
- Gone to the operating room for an attempt at hemorrhage control and
- Gone QUICKLY!
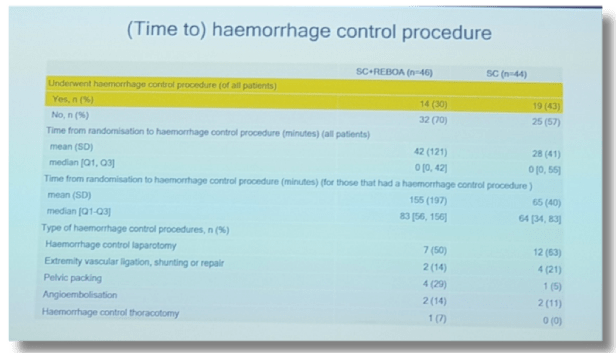
The Joint Statement ACS/COT ACEP best practice recommendations for REBOA clearly state that REBOA in Zone 1 should only be performed if the anticipated time to start of operation is less than 15 minutes. Even if the treating physicians chose not to follow these guidelines, it is hard to imagine what criteria they were using to include patients in this REBOA trial. Since no patient even came close to getting to the OR in a reasonable time in either group, then literally not a single patient should ever have been enrolled in this trial, in my opinion.
The UK-REBOA Trial Twitter results highlight 2 very important things to me so far:
- The trauma systems studied have major issues in getting this patient population expeditiously to the operating room regardless of whether REBOA is used or not and
- There is a severe lack of training and experience in those performing REBOA at most of these centers.
Most of these providers, despite their honest and best efforts, are clearly not experts in REBOA, even from their initial judgment standpoint about who might benefit from REBOA. However, this is not their fault, knowing from the published study protocol, that “Sites participating in the trial, most of whom had not previously used the technique, are provided with extensive training both prior to starting enrolment, and subsequently”. Perhaps it would have been better to have a minimum number of procedures completed for clinicians before they were allowed to recruit into the trial. Having been the Chief Medical Officer of a company selling a REBOA device and worrying all the time about novice users performing REBOA with the COBRA-OS®, it is absurd to me that patients would be recruited for an RCT in REBOA using providers that may never have even done REBOA on a real patient before.
To make matters worse about the apparent severe lack of experience and training of providers in this trial, enrollment was slower than expected (as stated in the published study protocol) and therefore the investigators added a further six major trauma centers in the middle of the trial and in the middle of a worldwide pandemic. How well trained do you think these additional providers were in these “second choice” trauma centers?
Ultimately, only 19/90 patients had the balloon inflated according to Dr Karim Brohi on Twitter, which is only 3 more than the total number of sites involved in the trial. 19 balloon inflations wouldn’t be beyond the annual realm for a single high volume trauma center using REBOA in the United States, and knowing our customers, they aren’t getting results like this. In what academic universe, can we say that this is the definitive evidence against REBOA? If the results of the trial had been positive for REBOA, I would be saying the exact same thing. The only takeaway message that I have at this point for the UK-REBOA trial is that the Learning Curve for REBOA can look pretty damn ugly if you don’t have the right technology, the right training, or the right patient selection.
Further musings…
As the broken record says, REBOA is only a tool in the toolbox for treating trauma patients. If there is an insistence on performing an RCT on every tool in that toolbox, then we better be prepared to investigate via RCT everything we have in our ambulances, emergency rooms, and operating rooms from REBOA devices all the way down to bandages. “It’s only necessary for risky new techniques or devices”, you say? Something like a tourniquet doesn’t need an RCT, does it? Well, I have personally amputated limbs from inappropriate tourniquet use in extremity trauma when direct pressure would have been adequate to stop bleeding and would have kept the limb alive. Why aren’t we beating on the tourniquet drum insisting that we stop all tourniquet use until we have level 1 evidence? Probably because common sense prevails and the education and training of the correct use of tourniquets should continue, while not throwing the baby out with the bath water. This is exactly what we should be doing with REBOA.
In my opinion, adequate RCT’s are almost impossible to perform in trauma patients because their injury patterns are so varied and there are very few generic treatments that apply to all hemorrhaging trauma patients. Studies involving medical devices, which require an acquired set of skills beyond the normal purview of trial investigators, are especially problematic to standardize and control in an RCT fashion. We can’t even definitively prove that administration of a medication improves outcomes in generic severe trauma (See tranexamic acid). Even if you choose to view trauma surgeons as nothing more than robotic technicians that perform exactly the same way every time, similar to giving a drug like tranexamic acid, you still can’t even be sure of a definitive result from an RCT.
In the end, if it makes sense for your patient and you are good at it, REBOA remains a great tool for non-compressible torso hemorrhage.